Author | |
Policy Lead | Chloe Gurney |
Version No. | 1.1 |
Date of issue | November 2022 |
Date to be reviewed | April 2026 |
Not controlled once printed | |
Introduction
Child safeguarding is everyone’s responsibility. Medisonal Limited is committed to ensuring individual rights are protected and promoted through eliminating all forms of abuse without discrimination. While it is not intended that Medisonal Ltd will be involved in the care of people under the age of 18. Staff must be aware that they still bear responsibility of being watchful for any risks to the safety and welfare of children, for example in the care of Medisonal Ltd’s adult patients, whether through family or household, or other circumstances, for example at patient’s places of work.
Children may be vulnerable to neglect and abuse or exploitation from within their family and from individuals they come across in their day-to-day lives. A child centred approach is fundamental to safeguarding and promoting the welfare of every child. A child centred approach means keeping in focus when making decisions about their lives and working in partnership with them and their families. All practitioners should follow the principles of the Children Acts 1989 and 2004 that state that the welfare of children is paramount and that they are best looked after within their families, with their parents playing a full part in their lives, unless compulsory intervention in family life is necessary.
Emergency services support is to be sought if risk is imminent to a child or if an individual assessing is unsure of the risk to a child.
The relevant local authority safeguarding policy is recognised in all of our services and will be referred to in conjunction with this policy.
Medisonal Limited operates across multiple local authority jurisdictions. If a staff member suspects a potential safeguarding issue has been committed against a child, it is their responsibility to liaise with the safeguarding lead / their manager immediately.
In this situation, a referral MUST be made immediately to the local authority safeguarding team based on where the child at risk is located. The NHS Safeguarding app will be used to achieve this, details for downloading the app can be found here NHS England » NHS England Safeguarding app
Policy Statement
Medisonal Limited is committed to ensuring individual rights are protected and promoted through eliminating all forms of abuse without discrimination. This includes:
- protecting children from maltreatment
- preventing impairment of children’s health or development
- ensuring that children are growing up in circumstances consistent with the provision of safe and effective care
- taking action to enable all children to have the best outcomes.
Scope
This policy and the procedures apply to all staff, including workers and independent sub-contractors.
Medisonal Limited are required to have a Safeguarding Lead responsible for guiding and supporting all staff when dealing with safeguarding children. The Safeguarding Lead for Medisonal Limited is Ayshen Lyoteva, in-house doctor.
Procedures
As a part of our commitment Medisonal Limited will:
- prevent and stop abuse or neglect wherever possible
- protect, maintain and uphold the human rights of children and young persons at risk
- eliminate discrimination
- take steps to deal with suspected abuse, bullying or exploitation of any kind whenever or wherever it may be found
- provide support, training and protection for everyone.
To meet our commitment, we will:
- ensure that everyone that works with us, for us or on our behalf is familiar with this policy and procedures and has access to the documents
- monitor the implementation of this policy and procedures and take any steps that are required to improve our practices
- ensure that effective procedures are in place for responding to complaints, concerns and allegations of suspected or actual abuse
- ensure that there are appropriate risk assessments in place
- ensure safe recruitment procedures including ID Checks, references and DBS checks are followed for every position we recruit to
- all individuals that work for us now or in the future, in any capacity, will be trained to Level 1 in Safeguarding, with clinical staff being trained to Level 2 and the Safeguarding Lead being trained to Level 3.
Children with Disabilities
Any child with a disability is by definition a ‘child in need’ under Section 17 of the Children Act 1989. The Disability Discrimination Act 2005 (DDA) and the Equality Act 2010 define a disabled person as someone who has “a physical or mental impairment which has a substantial and long-term adverse effect on his or her ability to carry out normal day to day activities”.
The Equality Act 2010 makes it unlawful to discriminate against a disabled person in relation to the provision of services. This includes making a service more difficult for a disabled person to access or providing them with a different standard of service.
Research suggests that children with a disability may be generally more vulnerable to significant harm through physical, sexual, emotional abuse and/or neglect than children who do not have a disability. Disabled children may be especially vulnerable to abuse for several reasons (e.g., they may be at increased likelihood of being socially isolated with fewer outside contacts than non-disabled children). Where there are concerns about the welfare of a disabled child, they should be acted upon in the same way as with any other child.
Types of abuse
Abuse is the violation of an individual’s human and civil rights. Abuse can be self-inflicted or inflicted by another person or persons. In the context of safeguarding, it is used to refer to any knowing, intentional or negligent act by another that causes harm or a serious risk of harm to another. Types of abuse include:
- Physical abuse that includes the deliberate hurting of a child who may present with:
- frequent injuries
- unexplained or unusual fractures or broken bones
- unexplained:
- bruises or cuts
- burns or scalds
- bite marks.
- Emotional abuse that includes persistent emotional maltreatment for which indicators include:
- children who are excessively withdrawn, fearful or anxious about doing something wrong
- parents or carers who withdraw their attention from their child, giving the child the ‘cold shoulder’
- parents or carers blaming their problems on their child
- parents or carers who humiliate their child (e.g., name-calling or making negative comparisons).
- Sexual abuse, including physical and non-contact activities. Indicators may include:
- displays of knowledge or interest in sexual acts inappropriate to age
- use of sexual language or have sexual knowledge unexpected in their age
- asking others to behave sexually or play sexual games
- physical sexual health problems, including soreness in the genital and anal areas, sexually transmitted infections or underage pregnancy.
- Sexual exploitation for money, power or status. Indicators may include:
- unexplained gifts or new possessions
- children who associate with other young people known to be involved in exploitation
- older boyfriends or girlfriends
- sexually transmitted infections or pregnancy
- changes in emotional wellbeing
- misuse of drugs and/or alcohol
- go missing for periods of time and/or regularly return home late
- regularly miss school or education, or do not take part in education.
- Neglect is a pattern of failing to provide for a child’s basic needs and may include the following indicators:
- homes that are dirty or unsafe
- left hungry and dirty
- inadequate clothing
- living in dangerous conditions (i.e., in the presence of drugs, alcohol or violence)
- angry, aggressive or self-harming behaviours
- failure to receive basic healthcare
- parents who fail to seek medical treatment when their children are ill or injured.
Contextual safeguarding
This is an approach to understanding and responding to young people’s experiences of significant harm beyond their families. Contextual Safeguarding, therefore, expands the objectives of child protection systems in recognition that young people are vulnerable to abuse in a range of social contexts.
As well as threats to the welfare of children from within their families, children may be vulnerable to abuse or exploitation from outside their families. These extra-familial threats might arise at school and other educational establishments, from within peer groups, or more widely from within the wider community and/or online. These threats can take a variety of different forms and children can be vulnerable to multiple threats, including exploitation by criminal gangs and organised crime groups, such as county lines, trafficking, online abuse, sexual exploitation and the influences of extremism leading to radicalisation. Extremist groups make use of the internet to radicalise and recruit and to promote extremist materials. Any potential harmful effects to individuals identified as vulnerable to extremist ideologies or being drawn into terrorism should also be considered.
Practitioners working with children and their families should consider whether wider environmental factors are present in a child’s life and are a threat to their safety and/or welfare. Children who may be alleged perpetrators should also be assessed to understand the impact of contextual issues on their safety and welfare.
Interventions should focus on addressing these wider environmental factors, which are likely to be a threat to the safety and welfare of a number of different children who may or may not be known to local authority children’s social care. Assessments of children in such cases should consider the individual needs and vulnerabilities of each child. They should look at the parental capacity to support the child, including helping the parents and carers to understand any risks and support them to keep children safe and assess potential risk to child.
Child sexual exploitation
Child sexual exploitation is a form of child sexual abuse. It occurs where an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child or young person under the age of 18 into sexual activity (a) in exchange for something the victim needs or wants, and/or (b) for the financial advantage or increased status of the perpetrator or facilitator.
The victim may have been sexually exploited even if the sexual activity appears consensual. Child sexual exploitation does not always involve physical contact, it can also occur through the use of technology. Child sexual exploitation takes different forms from a seemingly ‘consensual’ relationship where sex is exchanged for attention, affection, accommodation or gifts, to serious organised crime and child trafficking. Child sexual exploitation involves differing degrees of abusive activities, including coercion, intimidation or enticement, unwanted pressure from peers to have sex, sexual bullying (including cyber bullying) and grooming for sexual activity.
Children missing from care, home or education
Children running away and going missing from care, home and education is a key safeguarding issue. Current research findings estimate that approximately 25% of children and young people that go missing are at risk of serious harm.
There are particular concerns about the links between children running away and the risks of sexual exploitation. Looked After Children missing from their placements are vulnerable to sexual and other exploitation, especially children in residential care.
Children who go missing or run away from home or care may be in serious danger and are vulnerable to crime, sexual exploitation or abduction, as well as radicalisation. Healthcare professionals have a key role in identifying and reporting children who may be missing from care, home and school.
Missing children access a number of services provided by a range of health providers, including, Urgent Care Units, Emergency Departments, Genito-Urinary Medicine Clinics (GUM) and Community Sexual Health Services.
Health professionals should have an understanding of the vulnerabilities and risks associated with children that go missing. Staff should be aware of their professional responsibilities and the responses undertaken by the multi-agency partnership.
Child criminal exploitation and county lines
As set out in the Serious Violence Strategy (2018) published by the Home Office, where an individual or group takes advantage of an imbalance of power to coerce, control, manipulate or deceive a child or young person under the age of 18 into any criminal activity (a) in exchange for something the victim needs or wants, and/or (b) for the financial or other advantage of the perpetrator or facilitator and/or (c) through violence or the threat of violence, the victim may have been criminally exploited even if the activity appears consensual.
Child criminal exploitation does not always involve physical contact, it can also occur through the use of technology. County Lines is a term used to describe gangs and organised criminal networks involved in exporting illegal drugs into one or more importing areas within the UK, using dedicated mobile phone lines or other form of ‘deal line’.
They are likely to exploit children and vulnerable adults to move and store the drugs and money, and they will often use coercion, intimidation, violence (including sexual violence) and weapons. Potentially a child involved with a gang or with serious violence could be both a victim and a perpetrator.
This requires professionals to assess and support his/her welfare and well-being needs at the same time as assessing and responding in a criminal justice capacity. Professionals should always take what the child tells them seriously. If a professional is concerned that a child is at risk of harm as a victim or a perpetrator of serious youth violence, gang-related or not, the professional should wherever possible, consult with their line manager or the Safeguarding Children Team and make an immediate referral to Children’s Social Care.
So-called honour-based abuse
Honour based abuse is the term used to describe incidents of violence, including murder (“honour killings”) that have been committed in the belief that those actions will protect or defend the honour of the family and/or community. Such violence/abuse can occur when perpetrators perceive that a relative has shamed the family and/or community by breaking their honour code. The victims of such incidents are predominantly women, perceived to have behaved immorally and deemed to have breached the honour code of a family and/or community, causing shame. For young victims it is a form of child abuse and a serious abuse of human rights.
It can be distinguished from other forms of violence/abuse, as it is often committed with some degree of approval and/or collusion from family and/or community members. Women, men and younger members of the family can all be involved in the abuse. The Metropolitan Police definition of so-called honour-based violence is ‘a crime or incident, which has or may been committed to protect or defend the honour of the family and/or community. This type of violence and abuse includes physical, emotional, financial and sexual abuse of the victims. Professionals should respond in a similar way to cases of honour violence as with domestic abuse and forced marriage (i.e., in facilitating disclosure, developing individual safety plans, ensuring the child’s safety by according them confidentiality in relation to the rest of the family).
Forced marriage
A forced marriage is one where either or both parties do not (or in cases of people with learning disabilities, cannot) consent to the marriage and pressure or abuse is used against them.
Forced marriage, as distinct from a consensual ‘arranged’ one, is a marriage conducted without the full consent of both parties and where duress is a factor. Duress cannot be justified on religious or cultural grounds.
It is recognised in the UK as a form of violence against women and men, domestic/child abuse and a serious abuse of human rights. In 2004, the UK Government’s definition of domestic abuse was extended to include acts perpetrated by extended family members, as well as intimate partners. The pressure that is put on people to marry against their will may be physical (including threats, actual physical violence and sexual violence) or emotional and psychological (e.g., when someone is made to feel that they are bringing shame on their family). Financial abuse (taking away a person’s wages or not giving them any money) may also be a factor. If an individual does not consent or lacks capacity to consent to marriage, that marriage must be viewed as a forced marriage whatever the reason for it taking place. Capacity to consent can be assessed and tested but is time-and-decision specific. Professionals should respond in a similar way to forced marriage as with domestic violence and honour-based violence (i.e., in facilitating disclosure, developing individual safety plans, ensuring the child’s safety by according them confidentiality in relation to the rest of the family, completing individual risk assessments, etc.).
Female genital mutilation
Female genital mutilation (FGM) is a collective term for procedures, which include the removal of part or all of the external female genitalia for cultural or other nontherapeutic reasons. The practice is medically unnecessary, extremely painful and has serious health consequences, both at the time when the mutilation is carried out and in later life.
The procedure is typically performed on girls aged between 4 and 13, but in some cases, it is performed on new-born infants or on young women before marriage or pregnancy. FGM is practised in at least 29 countries across Africa, parts of the Middle East and Southeast Asia.
FGM is usually carried out on young girls between infancy and the age of 15, most commonly before puberty starts. It is estimated that 60,000 girls under 15 are at risk of FGM in the UK, and 137,000 women and girls in the UK have already been subjected to it.
Child protection procedures should be followed when there are concerns that a girl is at risk of, or is already the victim of, FGM. It comprises all procedures that involve partial or total removal of the external genitalia or other injury to the female genital organs for cultural or non-therapeutic reasons.
The practice is medically unnecessary and is linked to a number of forms of physical and psychological distress. There are also mandatory reporting procedures in place for health professionals in relation to FGM.
The duty to report applies in specific situations:
- A health professional is informed by a girl under 18 that an act of FGM has been carried out on her or
- A health professional observes physical signs which appear to show that an act of FGM has been carried out on a girl under 18 and they have no reason to believe that the act was necessary for the girl’s physical or mental health or for purposes connected with labour or birth.
Trafficking and Modern Slavery
The United Nations (Article 3 paragraph A of the Protocol to Prevent, Suppress and Punish Trafficking in Persons) defines Trafficking in Persons as the “recruitment, transportation, transfer, harbouring or receipt of persons, by means of the threat or use of force or other forms of coercion, of abduction, of fraud, of deception, of the abuse of power or of a position of vulnerability or of the giving or receiving of payments or benefits to achieve the consent of a person having control over another person, for the purpose of exploitation. Exploitation shall include, at a minimum, the exploitation of the prostitution of others or other forms of sexual exploitation, forced labour or services, slavery or practices similar to slavery, servitude or the removal of organs”.
Most children are trafficked and exploited for financial gain. Some trafficking is by organised gangs, in other cases individual adults trafficked children to the UK for their own personal gain. Exploitation includes children being used for sex work, domestic servitude, sweatshop and restaurant work, drug dealing and credit card fraud, begging or pickpocketing, benefit fraud, drug mules or decoys for adult drug traffickers, forced marriage, trade in human organs, and, in some cases, ritual killings. There are a number of circumstances that could indicate a child may have been trafficked to the UK and may still be controlled by the traffickers or receiving adults.
The National Referral Mechanism is a process set up by the Government to identify and support all victims of modern slavery following the implementation of the Modern Slavery Act, the mechanism through which the Modern Slavery and Human Trafficking Unit (MSHTU) collects data about victims. This information aims to help build a clearer picture about the scope of human trafficking in the UK. https://www.ecpat.org.uk/national-referral-mechanism
If You Suspect a Child is at Risk of Abuse
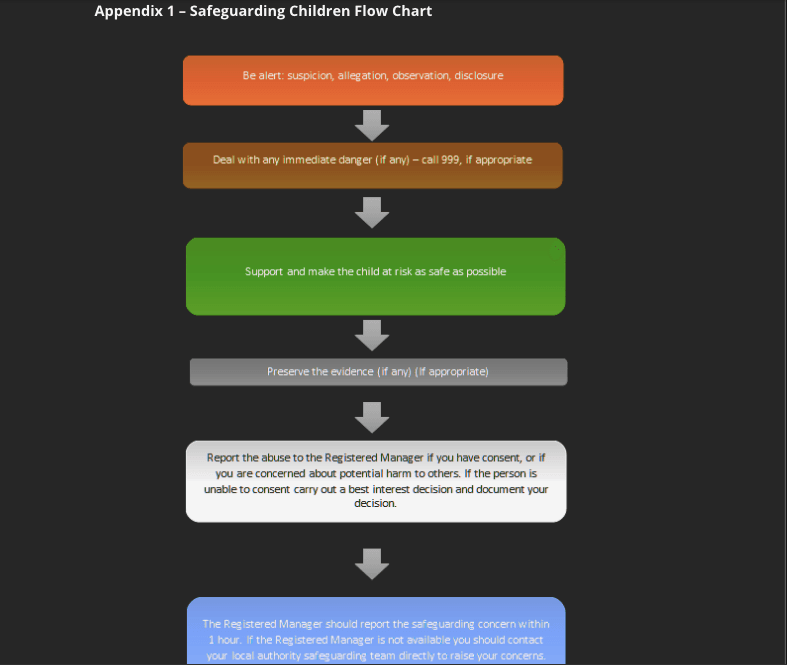
Where a child believed to be at risk of abuse is encountered or if they disclose or discuss potential abuse with you, it should be recognised that they may be describing abuse, albeit not explicitly. As a part of the initial assessment, you should try to establish the basic facts and question any unusual behaviours, speaking to the child alone if appropriate. If there is concern that a child is being abused or if they report abuse and/or neglect you should:
- listen
- take their allegation seriously
- reassure them that action will be taken to keep them safe.
The Safeguarding Lead must be informed immediately of any safeguarding concerns and further action will depend upon the circumstances of the case, the seriousness of the child’s allegation and the local multi-agency safeguarding arrangements in place. If the child is in immediate danger or is at risk of harm a referral should be made to children’s social care and/or the police.
The child should be kept informed of any action being taken, but, although it is important to maintain confidentiality, no promises should be made to keep the information a secret as this may need to be shared for their protection. It is then the role of social workers and/or the police to investigate cases and make a judgement on whether there should be a statutory intervention and/or a criminal investigation. If following this, there are then further signs of abuse and neglect, this should be reported and referred again. Following referral to a social worker a response should be received within one working day to confirm what further action may be needed.
Any safeguarding decisions should form a child centred approach, with the aim of keeping the child in focus and, where possible, working in partnership with them and their families.
Advice and assistance can also be sought from the NSPCC helpline: 0808 800 5000.
Children Exposed to Extreme Ideology
Extremism is defined in the Counter Extremism Strategy 2015 as the vocal or active opposition to our fundamental values, including the rule of law, individual liberty and the mutual respect and tolerance of different faiths and beliefs.
Extremism goes beyond terrorism and includes people who target the vulnerable, including the young by seeking to sow division between communities on the basis of race, faith or denomination; justify discrimination towards women and girls; persuade others that minorities are inferior; or argue against the primacy of democracy and the rule of law in our society.
Children and young people can be radicalised in different ways:
- They can be groomed either online or in person by people seeking to draw them into extremist activity. Older children or young people might be radicalised over the internet or through the influence of their peer network – in this instance their parents might not know about this or feel powerless to stop their child’s radicalisation.
- They can be groomed by family members who hold harmful, extreme beliefs, including parents/carers and siblings who live with the child and/or person(s) who live outside the family home but have an influence over the child’s life.
- They can be exposed to violent, anti-social, extremist imagery, rhetoric and writings which can lead to the development of a distorted world view in which extremist ideology seems reasonable. In this way they are not being individually targeted but are the victims of propaganda which seeks to radicalise.
A common feature of radicalisation is that the child or young person does not recognise the exploitative nature of what is happening and does not see themselves as a victim of grooming or exploitation. The harm children and young people can experience ranges from a child adopting or complying with extreme views which limits their social interaction and full engagement with their education, to young children being taken to war zones and older children being groomed for involvement in violence.
Radicalisation and the Prevent Strategy
Under Section 26 of the Counter-Terrorism Security Act 2015, healthcare professionals have a duty to have ‘due regard to the need to prevent people from being drawn into terrorism’. The Prevent strategy aims to reduce the threat of terrorism by preventing people from becoming terrorists or supporting terrorism and has three strategic objectives:
- respond to the ideological challenge of terrorism and the threat we face from those who promote it
- prevent people from being drawn into terrorism and ensure that they are given appropriate advice and support
- work with sectors and institutions where there are risks of radicalisation that we need to address.
Medisonal Limited will ensure that all staff understand and can comply with this duty through the implementation of mandatory prevention of radicalisation training. Staff will be expected to demonstrate:
- that they know what measures are available to prevent people from becoming drawn into terrorism
- how to challenge the extremist ideology associated with terrorism
- how to understand obtain support for people who may be being exploited by radicalising influences.
As a part of this strategy staff are also responsible for being:
- aware of their professional responsibilities in relation to the safeguarding of adults and children
- familiar with Medisonal Limited’s protocols, policies and procedures
- aware of who to contact to discuss any safeguarding concerns
- aware of the processes and support available following raising a concern
- aware of the current patient practice for patient confidentiality (see the Patient Confidentiality Policy for further information).
Changes to an individual’s behaviour indicative of potential radicalisation should be assessed for their reliability and significance by considering any:
- parental/family reports of unusual changes in behaviour, friendships or actions and requests for assistance
- patients/staff accessing extremist material online
- use of extremist or hate terms to exclude others or incite violence.
If staff are concerned that a vulnerable individual is being exploited, they should raise their concern with the Registered Manager and/or the Safeguarding Lead who will then consider referral to the relevant Local Authority or Regional Prevent Coordinator. Factors that can contribute toward an individual’s vulnerability and subsequent risk of radicalisation include:
- Identity crisis: radicalisers can exploit adolescents/vulnerable adults who may feel uncomfortable with their place in society and disconnected from their family and/or heritage by providing a sense of purpose or feelings of belonging.
- Personal crisis: can result in a sense of isolation, making a person vulnerable to radicalisation.
- Personal circumstances: individuals who feel their aspirations are likely to be undermined may translate into a generalised rejection of civic life and an adoption of violence as a symbolic act.
- Criminality: where a vulnerable individual becomes involved in a group that engages in criminal activity are more likely to be drawn into terrorist related activity.
- Grievances: the following may play an important part in the early indoctrination of vulnerable individuals:
- a misconception and/or rejection of UK foreign policy
- distrust of western media reporting
- perceptions that UK government policy is discriminatory (e.g., counter-terrorist legislation).
- Other factors:
- ideology and politics
- provocation and anger (grievance)
- need for protection
- seeking excitement and action
- fascination with violence, weapons and uniforms
- youth rebellion
- seeking family and father substitutes
- seeking friends and community
- seeking status and identity.
Information Sharing
Effective sharing of information between professionals and local agencies is essential for safeguarding and promoting the welfare of children and young people. Early sharing of information is the key to providing effective early help where there are emerging problems.
At the other end of the continuum, sharing information can be essential to put in place effective child protection services. Serious Case Reviews (SCRs) have shown how poor information sharing has contributed to the deaths or serious injuries of children (Working Together to Safeguard Children, 2018).
Fears about sharing information cannot be allowed to stand in the way of the need to promote the welfare and protect the safety of children. To ensure effective safeguarding arrangements:
- No professional should assume that someone else will pass on information which they think may be critical to keeping a child safe.
- If a professional has concerns about a child’s welfare and believes they are suffering or likely to suffer harm, then they should share the information with local authority children’s social care.
Further information relating to information sharing can be found in the Information Governance and Client Confidentiality Policy. Where sharing concerns with parents could increase risks to a child, for example sexual abuse within the family when there is a danger of the parents silencing the child, staff should make the referral without informing the parents and record this in the care plan.
Children have a right to be told what is going on. They should not be given promises that cannot be kept. Their views and wishes should be taken into consideration, in accordance with their age and developmental status. Clients and children should be made aware that confidentiality can never be absolute, as staff have a duty to ensure they are protected from harm.
Safeguarding Remotely
The same principles of safeguarding apply whether services are being performed in person or remotely. However, staff should be aware that identifying children at risk of abuse may be more difficult in a remote environment. If there are any concerns as to the welfare of the child, consideration should be given as to whether the remote service is an appropriate approach in that situation. Any concerns should be referred to the Safeguarding Lead for advice and assistance.
Staff Conduct
Medisonal Limited will not tolerate any staff, worker, or other person engaged to support or provide services to, or on our behalf to have:
- behaved in a way that has harmed, or may harm, a child or young person
- possibly committed a criminal offence against, or related to, a child or young person
- behaved towards a child or young person in a manner that may indicate they are unsuitable to work in a position of trust.
Any staff member identified to behave in such a way as to indicate one or more of the above statements, either within their work or as a consequence of actions within their personal life may be subject to disciplinary action. Identification of such incidents can come from various different sources. Medisonal Limited will take prompt action to investigate any allegations made and will take any actions necessary to protect our clients and those that work with us, for us and on our behalf. Resultant actions can/may include a member of staff being suspended, and possibly dismissed.
All allegations will be reported to the CQC without delay, as is required. Where the allegation is made against a healthcare professional we will liaise with and report to the relevant professional body.
Additionally, Medisonal Limited has a duty to refer staff to the Disclosure and Barring Service (DBS) if they have:
- Satisfied the harm test, i.e., that the Company believes that the staff member(s) may:
- harm a child or vulnerable adult
- cause a child or vulnerable adult to be harmed
- put a child or vulnerable adult at risk of harm
- attempt to harm a child or vulnerable adult; or incite another to harm a child or vulnerable adult.
- Received a caution or conviction for a relevant offence.
A relevant offence for the purposes of referrals to DBS is an automatic inclusion offence as set out in the Safeguarding Vulnerable Groups Act 2006 (Prescribed Criteria and Miscellaneous Provisions) Regulations 2009 and the Safeguarding Vulnerable Groups.
Broadly speaking these offences include all sexual offences, all offences involving children, most prostitution offences and murder. If you are unsure, contact the HR Department for guidance.
If the above conditions have been met and the Registered Manager will conclude that the investigation conducted shows that the staff member concerned has a case to answer, a referral must be referred to DBS.
Staff Training
All staff and third parties working or volunteering with Medisonal Limited will be required to undertake an induction that includes mandatory training on the safeguarding of children as well as the Prevent strategy for radicalisation.
This will then need to be updated at least every 3 years.
Monitoring
The Leadership Team will receive regular reports from the appointed Safeguarding Lead to include the following content where applicable:
- numbers of staff attending and completing training
- numbers of safeguarding referrals made to the local authority and CQC
- lessons learned and changes effected as a result of safeguarding issues.
Related Policies and Procedures
Equality and Diversity Policy and Procedures
Information Governance and Record Keeping Policy and Procedure
Mental Capacity Act and DoLS Policy and Procedures
Recruitment Policy and Procedures
Staff Training and Induction Policy and Procedures
Whistleblowing Policy and Procedures
Legislation and Guidance
Children Act 1989
Children Act 2004
Counter Extremism Strategy
Disability Discrimination Act 2005
Equality Act 2010
Mental Capacity Act 2005
Public Interest Disclosure Act 1998
Modern Slavery Act 2015
United Nations Protocol to Prevent, Suppress and Punish Trafficking in Persons
Home Office: Revised Prevent duty guidance: for England and Wales 2021: https://www.gov.uk/government/publications/prevent-duty-guidance/revised-prevent-duty-guidance-for-england-and-wales
Home Office Serious Violence Strategy (2018) published by the Home Office,
NICE Guidance: https://www.nice.org.uk/guidance/health-and-social-care-delivery/safeguarding
Care Quality Commission: https://www.cqc.org.uk/sites/default/files/20150710_CQC_New_Safeguarding_Statement.pdf
HM Government: What to do if you’re worried a child is being abused; advice for practitioners, 2015 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/419604/What_to_do_if_you_re_worried_a_child_is_being_abused.pdf
Working Together to Safeguard Children, 2018
Compliance
Safe | S1: How do systems, processes and practices keep people safe and safeguarded from abuse? S2: How are risks to people assessed and their safety monitored and managed so they are supported to stay safe and their freedom is respected? |
Responsive | R2: How are people’s concerns and complaints listened and responded to and used to improve the quality of care? |